Amyloidosis and Diabetes in a dog
History: A twelve year old castrated male Miniature Schnauzer was presented with diabetic ketoacidosis and a 48 hour history of vomiting, polyuria, and polydypsia.  The dog also had a chronic history of urinary tract infection.  The dog died of cardiac arrest.
Gross Lesions: (no gross pictures)
Heart: Â Endocardiosis
Lungs: Â Diffuse congestion and edema
Eye: Â Corneal inclusion cyst
Urinary bladder: Â Cystitis
Liver: Â Multifocal nodular regeneration
Gall Bladder: Â Mucocoele
Histopathology:
Kidneys:  The glomerular tufts are hypocellular with increased mesangium and amyloid. Glomeruli were positive for amyloid by Congo Red stain showing an orange material that glows green with polarized light. Amyloid is present globally in some glomeruli and segmentally in others. In some cases amyloid is admixed with collagen in the same glomerulus.
Bowman’s capsules have thickend basement membranes (PAS positive) and the parietal epithelium of Bowman’s capsule is multifocally lined by cuboidal epithelium.  Occasional tubules contain eosinophilic granular casts.  There is increased amounts of fibrous tissue in the cortex and medulla.
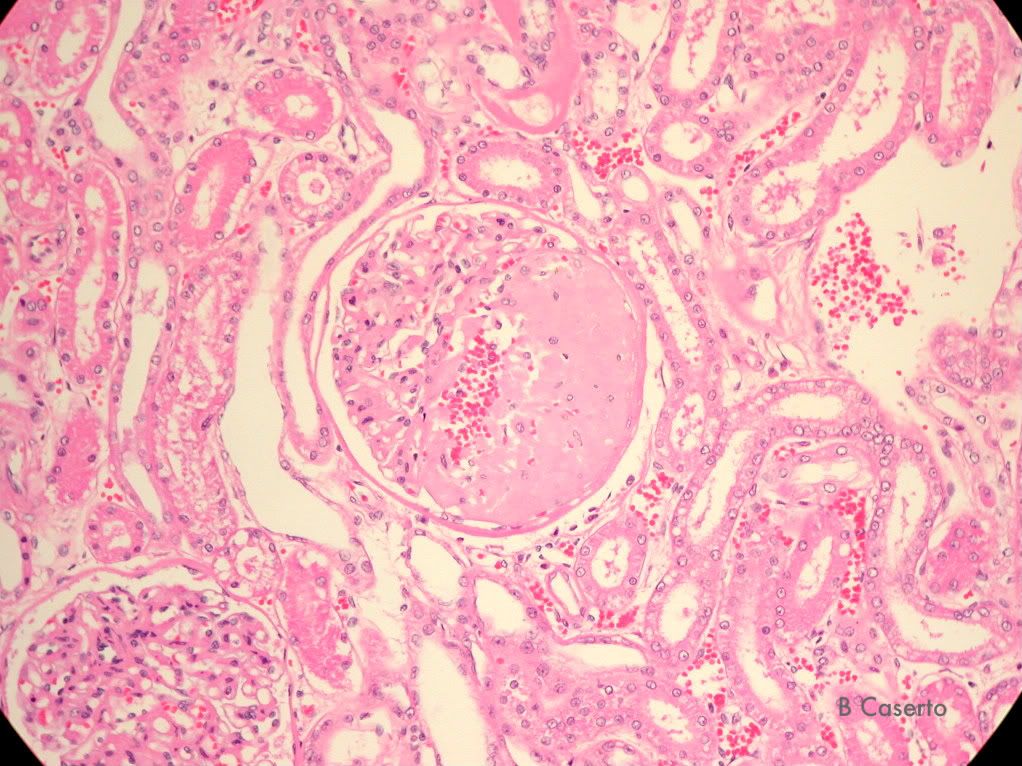
Kidney: Glomerular tuft is thickened (segmentally) with eosinophilic material (amyloid)
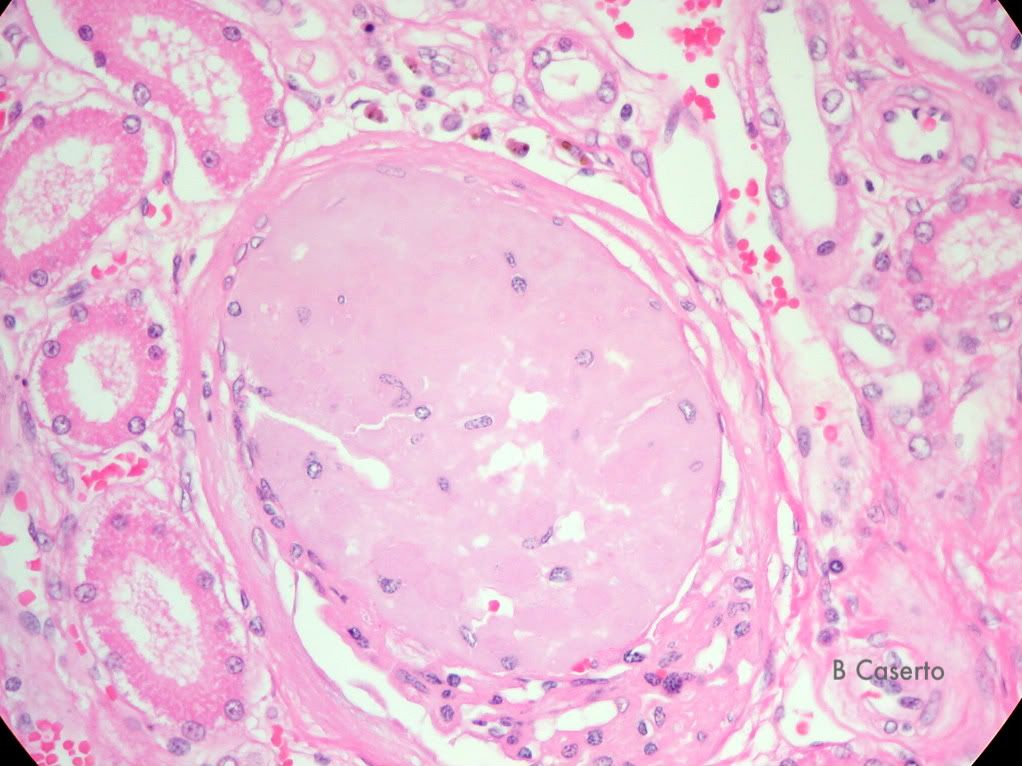
Kidney: Glomerulus is completely thickened (globally) with eosinophilic material (amyloid)
Kidney: Glomerulus with Congo Red stain- orang/red = amyloid

Kidney: Multiple Glomeruli: Polarized light and Congo Red stain- Apple green bi-refringence = amyloid
Eye:  There is a small cyst lined by stratified squamous epithelium within the cornea.

Cornea: Epithelial inclusion cyst
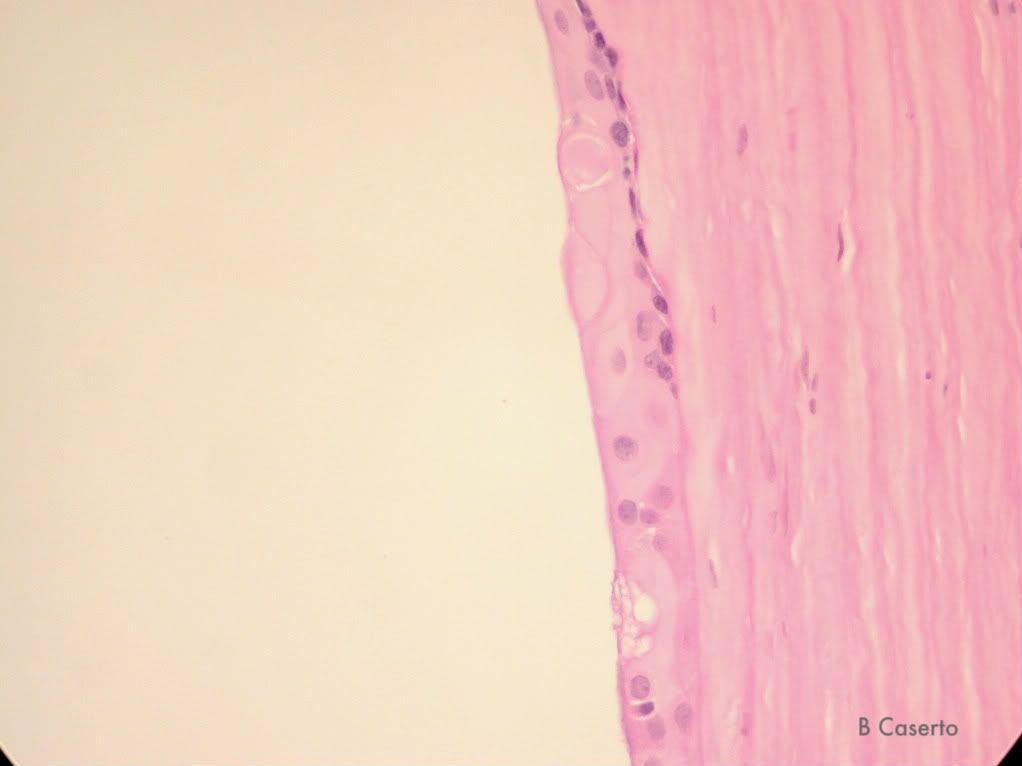
Cornea: Interior lining of the cyst- lined by cuboidal epithelium
Liver:  Multifocally hepatocytes contain moderately sized clear lipid vacuoles, and scattered Kupffer cells contain hemosiderin.  There are numerous hepatocytes with yellow/brown cytoplasmic pigment (bile). There are multifocal coalescing areas of nodular hyperplasia with variably sized hepatic lobules.
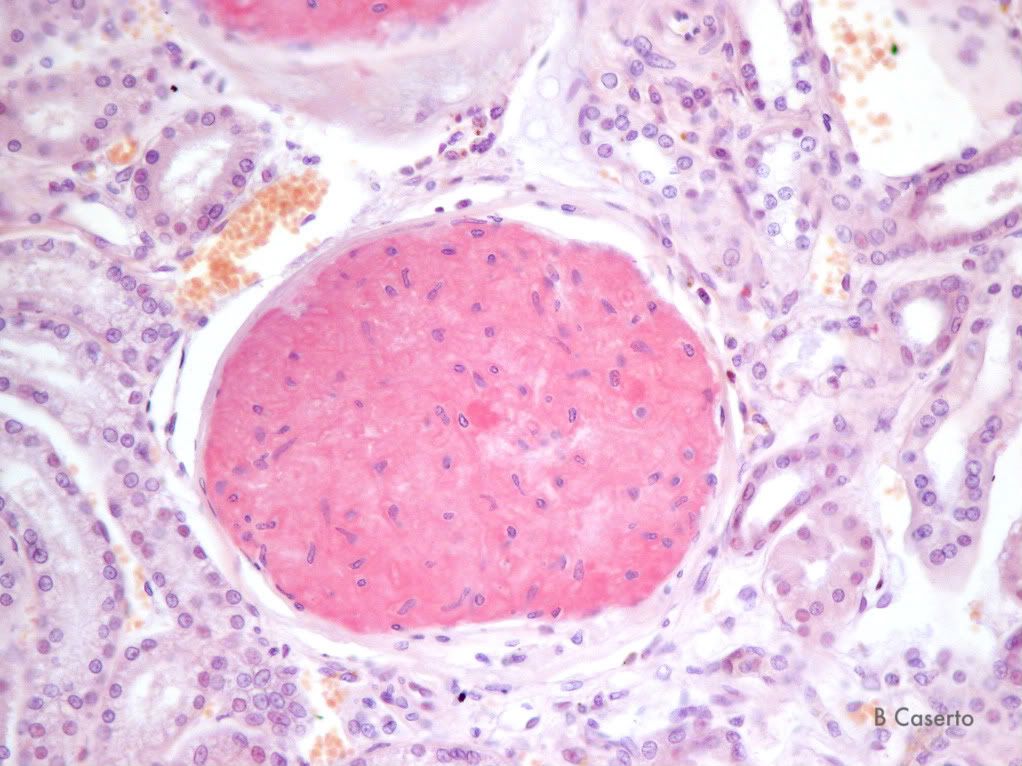
Heart:  In the atria the arteriolar walls are thickened with an eosinophilic material resembling amyloid.  The smooth muscle cells of the tunica media are vacuolated and the lumen is narrowed in many arterioles.  The aortic valve is focally expanded by a pale basophilic matrix of mucinous material.  The base of the valve is replaced by chondrocytes within lacunae surrounded by basophilic cartilaginous matrix.
Spleen:  Small arterioles contain vacuolated and swollen smooth muscle cells with replacement by amyloid and mineralization.
Lung:  In multifocal areas the alveoli and small bronchi contain large numbers of degenerate and intact neutrophils with small amounts of fibrin.
Pancreas:  Diffusely there are fewer Islets than normal and the ones that are present are small, with few vacuolated cells.
Gall bladder:  The glands of the gall bladder mucosa are dilated and hypertrophied and filled with amphophilic material.  The mucosa is covered with a layer of amphophilic material approximately 10x the thickness of the gall bladder wall.
Diagnosis:
1. Kidneys: Â Amyloidosis, multifocal, global and segmental
2. Eye, cornea: Epithelial inclusion cyst, focal
3. Heart and spleen: Â Arteriolar medial degeneration and amyloidosis
4. Heart, aortic valve: Â Endocardiosis, focal, severe
5. Lung: Bronchopneumonia, mild, multifocal
6. Pancreas: Â Pancreatic Islet atrophy and degeneration
7. Gall bladder: Â Mucocoele
Comment:
The most significant lesion (to the dog) is the loss of Islets of Langerhans in the pancreas. Â This ultimately led (presumably) to the urinary tract infection, and to the acute crisis of diabetic ketoacidosis. Â Uncontolled diabetes mellitus can explain the clinical signs noted in the history (Polyuria/polydypsia, vomiting). Â The photomicrographs highlight the diagnosis of amyloidosis in the glomeruli using Congo Red and polarized light (apple green bi-refringence). Â The amyloid is presumably AA type resulting from the chronic urinary tract infection. Â In this case amyloid was found in the glomeruli and in the small arterioles of the heart and spleen. Â The cause of the bronchopneumonia is unknown. Â The rest of the lesions were considered incidental findings.
Amyloidosis can be subdivided into 2 common subtypes in domestic animals.  One is the AA type in which the amyloid fibrils are derived from serum amyloid A (SAA) – a positive acute phase protein.  IT is produced by the liver under the influence of acute inflmmatory cytokines IL-1, and IL-6.  The second type is AL, which is derived from the light chains of immunoglobulins (amyloid light-chain), which is produced by plasma cells in certain autoimmune disease, and multiple myelomas, or chronic activation of humoral immunity.
Other types of amyloid proteins (other than AA and AL) include:
AB (beta) amyloid- age related neurodegenerative change.
IAPP- Islet amyloid polypeptide- secreted by beta cells in the pancreas. Found in Islet amyloidosis. Â This can lead to development of
AI- Apolipoprotein AI- Found in the pulmonary vasculature of aged dogs
Prion Diseases-Â CWD , Scrapie, BSE, Mink and feline spongioform encephalopathy.
References:
Snyder PW. Diseases of Immunity. Chaper 5 in Pathologic Basis of Veterinary Disease, 4th ed, eds McGavin DM, and Zachary JF. Â Mosby, Inc, St Louis Missouri. Â 2007
没有评论:
发表评论